2.5. Application Example 2: Child Immunization¶
2.5.1. Overview¶
This example reproduces some of the analysis originally published in Spielauer & Dupriez (2020) - a paper studying and projecting child vaccination in Nepal. In a set of what-if scenarios, we project the change of immunization rates resulting from ongoing socio-demographic changes (our base scenario; we use the same base scenario as in Example 1) as well as from hypothetical improvements in closing gaps between ethnic groups and regional gaps in immunization, and improvements in prenatal care which is an important predictor for immunization. Unlike the first example, which - as one of the studied downstream effects - shows the effect of changes in primary education on immunization, in the scenarios of this exercise we leave education outcomes unchanged but modify the following parameters:
- Region: regional differences in prenatal care and immunization.
- Ethnicity: ethnic differences in immunization.
- The effect of mothers’ education on prenatal care
The presented analysis is an example of convergence scenarios. Convergence scenarios close the gap between population groups by a transition of group specific regression coefficients (in our case odds ratios) to the coefficients of the group with the currently highest outcome. The scenarios mimic policy goals of targeting disadvantaged groups (e.g. low castes) and removing regional differences over a set period of time.
2.5.2. Scenarios¶
- The base scenario uses the default parameters
- Closing regional gaps: In this scenario, regional gaps in prenatal care and immunization are closed over a transition period of 10 years.
- Closing gaps between ethnic groups: In this scenario, ethnic gaps in immunization are closed over a transition period of 10 years.
- Closing regional gaps and gaps between ethnic groups: In this scenario, both gaps are closed over a transition period of 10 years.
- Closing regional gaps and gaps between ethnic groups (as above) as well as the gaps in prenatal care by mother’s education. In this scenario, the education of mothers (after the transition period) has no effect on prenatal care and all women receive prenatal care as currently women of the highest education group.
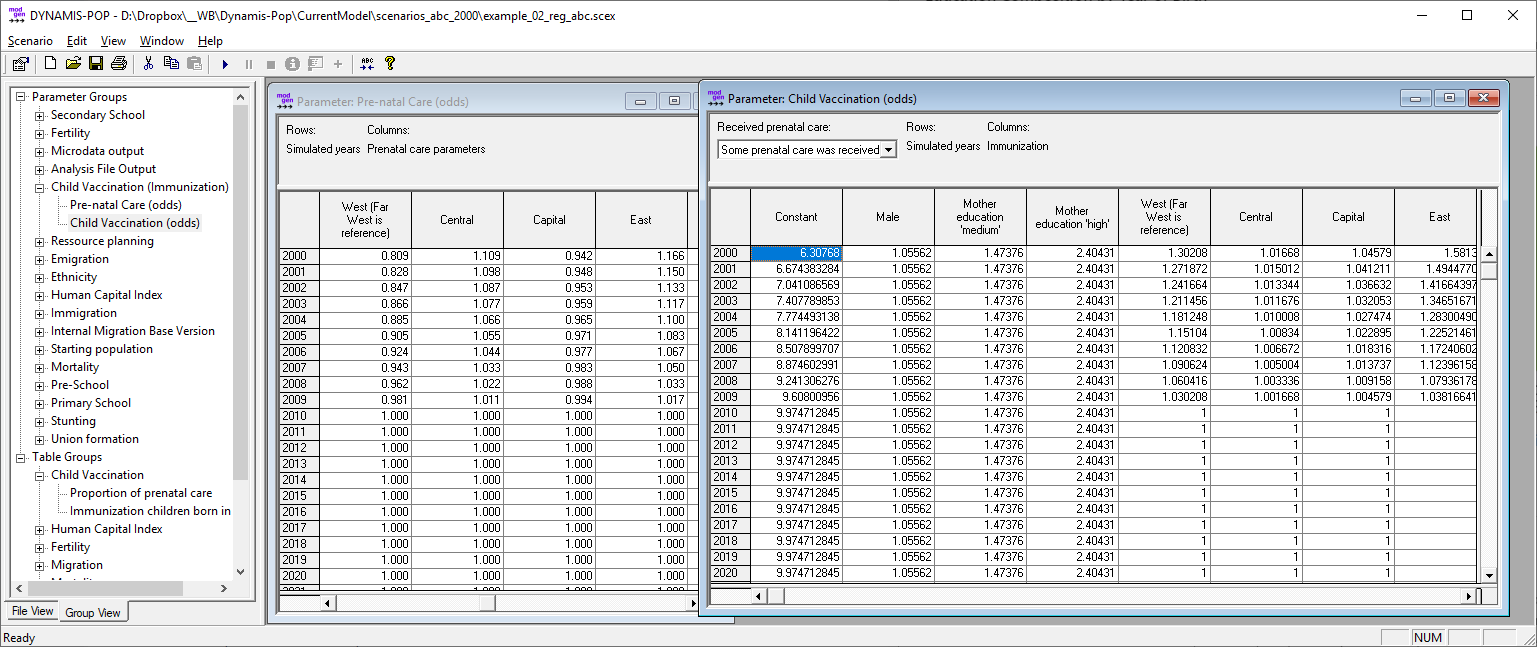 Figure: Scenario settings to close regional gaps. For prenatal care all odds ratios converge to 1 (as they are all initially lower than 1 which is the reference). For immunization, all odds ratios converge to 1 and the constant term is increased by the factor of the highest initial odds ratio
Figure: Scenario settings to close regional gaps. For prenatal care all odds ratios converge to 1 (as they are all initially lower than 1 which is the reference). For immunization, all odds ratios converge to 1 and the constant term is increased by the factor of the highest initial odds ratio
Other Settings:
- Fertility: we use the refined model without alignment and trends. The refined model accounts for fertility differentials by education.
- Immigration and Emigration are switched off for this analysis.
- As we project immunization until the 2050 birth cohort, the simulation horizon was set to 2051.
2.5.3. Simulation Results¶
2.5.3.1. Prenatal Care¶
Prenatal care is highly associated with primary education. The improving educational composition of mothers leads to a modest improvement of overall rates. Closing regional gaps further increases prenatal care rates. Removing the discrepancies by education would show the greatest effect by far.
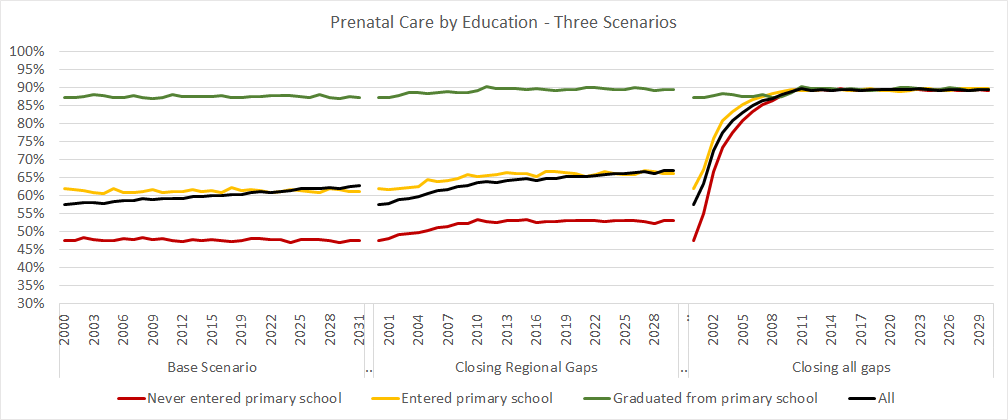 Illustration based on output table: “Prenatal Care”
Illustration based on output table: “Prenatal Care”
2.5.3.2. Immunization¶
Like prenatal care, also immunization rates are highly associated with primary education. The improving educational composition of mothers leads to a modest improvement of overall rates. The largest effect of the studied single measures would result from closing the ethnic gaps.
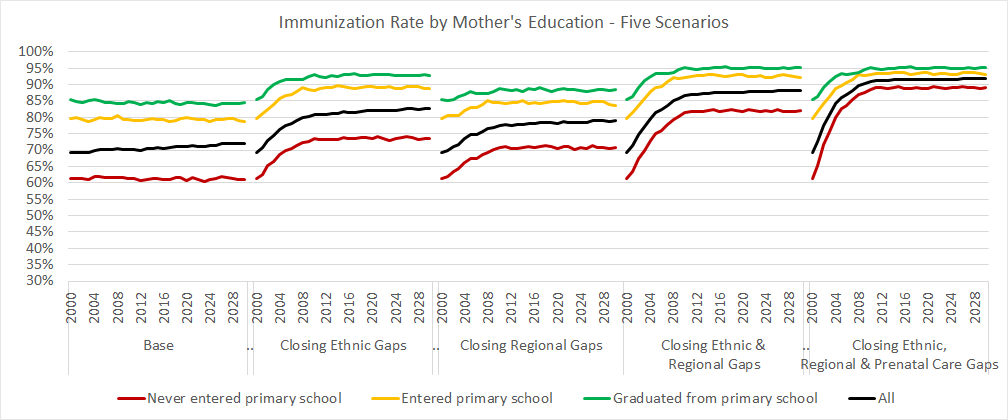 Illustration based on output table: “Immunization”
Illustration based on output table: “Immunization”
Comparing the scenarios allows decomposing the effects of each change on the aggregate outcome.
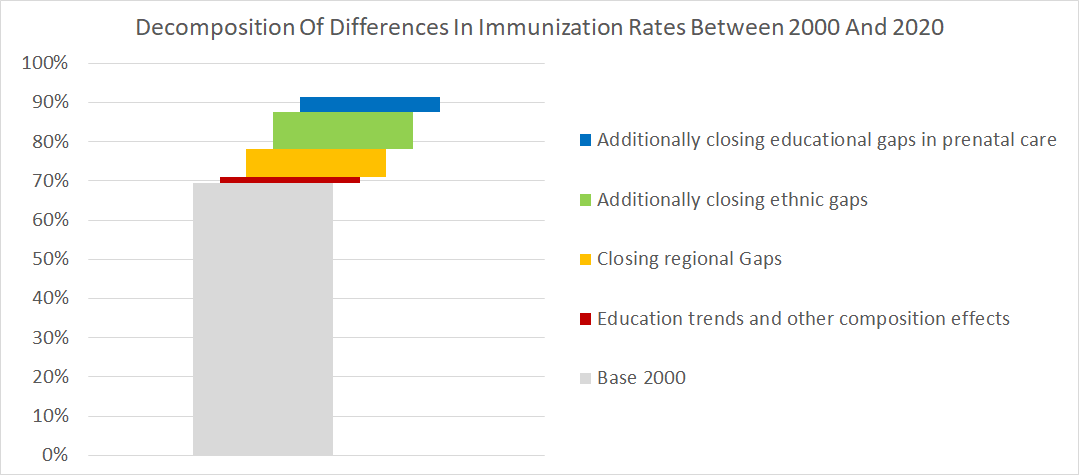 Illustration based on output table: “Immunization”
Illustration based on output table: “Immunization”